|
|
|
Referring Your Patients to a Chiropractor: A Guide for MDs/ DOs and Other Health Professionals
|
|
|
|
|
|
Prepared by John J. Collins, DC Springbrook Chiropractic
& Natural Health Center
Newberg, OR 97132
503-538-0618
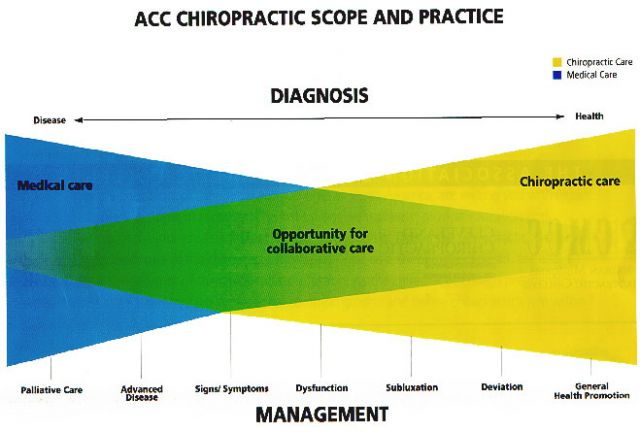
Important background information for medical providers:
In
Oregon (just like all 50 states) chiropractors are legally classified
as "Primary-contact" health care providers. There is NO legal requirement for
medical referral. Chiropractors are legally responsible and liable for:
1- Establishing a 'diagnosis' and plan for any 'condition/s' they intend to treat.
2- Managing the patient's case appropriately as per the state CHIROPRACTIC (not medical!) laws and statutes.
3-
Referring the patient to other health care providers when necessary
(i.e. where there is reason to believe that lack of appropriate medical
evaluation and/or care will result in significant and/or lasting
detrimental health effects). All chiropractors are
sufficiently-educated and prepared to reasonably identify patients with
conditions that are outside of the chiropractor's scope of practice.
BUT, MDs/DOs should be aware that not all chiropractors are the same
and this is a good thing, trust me! There are actually various
'unofficial' sub-specialties within the chiro profession. Much of the chiropractic profession (including me) are resisting the "commodification" of healthcare known as 'evidence-based medicine' and we will likely continue to defend our right to practice clinically-diverse, patient-centered care. MDs and DOs
should remain open to working with any and all types of chiropractors, as these relationships will ultimately result in improved health for your patient.
More background: As you may
know, lots of people visit chiropractors! Perhaps 15-18% of the
population attends a chiropractor each year and approximately 50% of
the population have seen a chiropractor at some time. Over a 7 year period from 2000-2006 I myself
rendered care to over 1200 different patients...this
is approximately 4% of the Greater Newberg area! And, there are 9 -10 other chiropractors
in the area, so perhaps 30-40% of the people in the Greater Newberg
area have visited a chiropractor during those years!
Let's Collaborate!
|
|
Common reasons for chiropractic care/ treatments used/ typical scenarios
-Common Reasons Patients Present To My Office
1-Acute
and chronic spine and/or paraspinal pain of the pelvic, lumbar,
thoracic, cervical or occipital region of traumatic or non-traumatic
origin (You need not absolutely rule out pathological/organic cause,
the chiropractor can do this for you).
2-Injuries to spine and/or
paraspinal muscles/connective tissues such as: 'Whiplash'-like injuries
or lumbar/pelvic/sacro-iliac 'sprain/strains'. Also- shoulder pains are
common.
3-Radicular pain, parasthesia, referred-somatic pain or numbness to the upper and/or lower extremities.
4-Headaches
of all shapes and sizes, but most notably those wherein the patient has
identified some sort of NMS connection in their own observations.
5-Sports injuries of all types.
6-
Various states of ill-health, dysfunction and/or 'dis-ease' wherein
spinal biomechanical malfunction and concommitant neurological
disturbances MIGHT be contributing factors.
i.e. Otitis media, menstrual disturbances, digestive problems, osteo-arthritis, emotional dysfunction, asthma etc.
7-Overall health promotion.
-Treatments Used
1-Chiropractic spinal 'adjustments' (these are primarily manipulation-like techniques).
2-Other soft-tissue mobilization techniques.
3-Modalities such as heat, cold, ultrasound, high volt galvanic current, interferential current.
4-Massage.
5-Exercise and 'spinal-hygiene' instruction.
6-Dietary and healthful life-style counseling and group classes.
7-Foot orthotics.
-Typical Scenarios- Each case is unique, as my approach tends to be more patient-centered than condition-centered.
-23
year old male electrician with recent-onset of non-debilitating left
sacro-iliac pain which he attributed to "twisting wrong" when pulling
electrical wire. Diagnosis was traumatic sacro-iliac joint subluxation
(non sprain/non strain)
Patient was treated 3 times with excellent
reduction of pain. He was strongly advised to quit his horrific habit
of chewing tobacco. He was advised to attend a spinal ergonomics and
exercise class but never attended. He was additionally advised to get
regular quarterly spinal checks but has chosen to come in on occasion
when he feels his 'back is out'.
-53 Year old male with acute,
markedly debilitating lumbo-sacral pain with referred pain to lower
leg. Injury came from lifting heavy object. Diagnosis was moderate
strain/sprain of lumbo-sacral region and subsequent spinal joint
dysfunction confounded by moderate-marked L5-S1 disc spondylosis.
Patient was treated 3 times per week for two weeks and 2 times per week
for 2 weeks with good reduction of symptoms. Patient was stationary and
at nearly pre-injury status in 6 weeks when he was released from
therapeutic care. He continues on with voluntary monthly 'maintenance
adjustments in order to maintain a higher biomechanical function, by
keeping developing subluxation/fixations at bay.
-48 year old
deconditioned female smoker was 'rear-ended' by another vehicle. She
suffered from markedly debilitating pain and stiffness in
occipital/cervical/thoracic region, headache, bilateral upper extremity
pain with bilateral C8 domain parasthesia, occasional dizziness and
photophobia, anxiety, emotional lability, acute lumbo-sacral pain with
bilateral, intermittent full-foot parasthesia and/or numbness. The
diagnosis was marked, acute, traumatic 'whiplash-like' sprain/strain to
multiple connective tissues of the spine and paraspinal region et. al.
This patient's healing was 'managed' with chiropractic care over a 5
month period. The initial phase consisted of more-frequent visits to
palliate/ameliorate/mitigate her severe symptoms. The second phase
consisted of less-frequent office-visits emphasizing the restoration of
normal biomechanics and beginning of rehabilitative and re-conditioning
activities. The third phase emphasized the re-conditioning aspect. Her
results were excellent and the patient's satisfaction with care was
extremely high. She was found to be 'maximum medical improvement' after
approximately 5 months/30 treatments even though she was only 95% back
to her pre-injury status. This patient may never be 100%, such is the
very serious nature of these types of spinal 'soft tissue' injuries.
-Pregnant
female: She presents at 18 weeks with only mild SI pain...she is
feeling tight muscles in low back. She is diagnosed with mild SI
postural strain with underlying subluxation dysfunction due to biomechanical changes of pregnancy. She
is adjusted and advised to get checked monthly throughout her
pregnancy. She does so and has a completely uncomplicated pregnancy and
birth.
-This is just a short sample!
|
|
Insurance Coverage/ Payment Issues/ How To Refer
Statistically,
a growing number of people are obtaining "chiropractic benefits".
However, much of it is unreasonable/irrational managed care coverage. I
only participate in a very limited number of PPOs (2 exactly).
I have found that participation in MCOs have resulted in lower quality of care and I prefer to work directly with a cash-paying patient. Most patients at my office do not have so-called chiropractic
"coverage"! As a result, our fees are very reasonable and fully disclosed before
care commences (ie. initial exam:$100, x-rays(if needed):$50-100, typical
treatment $45-85. My staff will either already know or be able to
quickly determine precisely what coverage (if any) is available. Leave it to us!
How To Refer The Patient: (First,
there is a difference between a 'referral' and 'prescription'! I am no
longer honoring "prescriptions") [i.e. please treat 3 times for SI dysfunction etc.] I have grown to believe that MDs/DOs have no more
business "prescribing" chiropractic care than they do "prescribing"
dental care! However, given that the scope of MDs and chiros overlap,
it is appropriate for an MD to request that a chiro limit their care to
a particular issue/problem/symptom. I will usually gladly comply with
your request.
Typical referral requests might be worded as follows:
1)
Scenario #1: (full referral for chiropractic management) example---
"Dr. Collins, please evaluate and treat patient for her chronic
headaches/backaches/injuries etc., send initial and progress reports."
2)Scenario
#2 (co-management, MD is primary) example--- "Dr. Collins, please evaluate
and treat patient limit eval and treatment to xyz symptoms/condition.
Send initial and progress report." (If I disagree with your rationale
for requesting a limited scope, I will make my opinion known to you
without usurping your clinical authority, but you need to be able to
defend your clinical reasoning.)
3) Scenario #3 ("prescription" for
chiropractic care): example---"Dr. Collins, please treat patient with
spinal manipulation for S.I. dysfunction with 3 treatments." Now,
imagine referring your patient to a dentist and advising the dentist
which teeth needed to be filled and which ones needed crowns etc???
Please do not send me a patient with a "prescription", I will NOT honor it, thanks. Remember, I humbly and gratefully accept your thoughtful referrals, and will do my absolute best with each and every patient.
Sincerely,
John J. Collins, DC
Newberg, OR
|
|
|